
Gülşah Kayserilioğlu 1, Sema Koçaşlı 2
1 Çankırı Karatekin University Eldivan Vocational School of Health Services, Çankırı, Turkey
2 Ankara Yıldırım Beyazıt University, Faculty of Health Sciences, Surgical Nursing, Ankara, Turkey
Received: 4 June 2024
Revised: 12 June 2024
Accepted: 12 Jun 2024
Published: 12 Jun 2024
Corresponding author:
Gülşah Kayserilioğlu.
Lecturer, Çankırı Karatekin University Eldivan Vocational School of Health Services, Çankırı, Turkey.
gulsah.kayserilioglu@gmail.com
| doi: 10.5281/zenodo.11543205 |
ABSTRACT
| The aim of this systematic review and meta-analysis study is to examine the effect of laughter therapy applied to adult patients on anxiety, stress, sleep and quality of life. The study was conducted in systematic review and meta-analysis design. Searches were conducted between March 2013 and March 2023, in Web of Science, Pubmed, Science. Direct, Scopus, Cochrane, Proquest and YÖK-National-Thesis-Center databases. The data were synthesized by meta-analysis methods using the Comprehensive Meta-Analysis (CMA) 3.0 program. 16 studies were included in meta-analysis, 7 of which were randomized controlled and 9 of which were quasi-experimental, published in 2013-2023. The total sample size of the studies was 1276 (control: 600 and laughter therapy: 676). The combined results of the studies showed that the sleep quality in the laughter therapy group was statistically significantly higher than the control group (g= -2,00, p=0.02); the mean anxiety score of the laughter therapy group (g= -1.93, p=0.03), and the stress level of the laughter therapy group (g= -1.70, p=0.02) was found to be less than the control group. According to the results of the study, the quality of life of the laughter therapy group was found to be statistically significantly higher than the control group (g= 0.71, p=0.009). This study showed that laughter therapy applied to adult patients is effective in increasing sleep quality and life quality, and also effective in reducing the level of stress and anxiety. |
Keywords:
Adult patients, laughter therapy, laughter yoga
Cite as:
Kayserilioğlu G, Koçaşlı S. The Effect Of Laughter Therapy Applied To Adult Patients On Anxiety, Stress, Sleep And Quality Of Life Systematic Review And Meta-Analysis. Acta Med Eur. 2024;6(3):79-91.
doi: 10.5281/zenodo.11543205
INTRODUCTION
Acute or chronic diseases are sources of both physiological and psychological stress that affect the adaptation processes of the individual (1-5). The incidence of chronic and acute diseases is increasing in the world and in our country. According to the data of the World Health Organization (WHO), 41 million people die every year from non-communicable diseases and related complications, which corresponds to 74% of all deaths worldwide. When Turkish Statistical Institute (TSI) data is examined, 40% of deaths are caused by cardiovascular system diseases, 20% by cancers, 12% by respiratory system diseases, and 5% by endocrine-nutritional and metabolic diseases in Turkey (6-7). The gradual increase in the rate of loss of function due to diseases and their complications negatively affect individuals’ adaptation to the disease process and their quality of life (4,5,8-10). The disease process itself and the inability to adequately adapt to this process can cause various symptoms such as increased anxiety, pain, nausea-vomiting, changes in bowel habits, various stress responses (changes in blood glucose level, blood pressure, etc.), sleep problems, mood disorders and inadequate ventilation. When these symptoms cannot be managed effectively, individuals’ adaptation to their treatment is delayed, the duration of treatment and hospitalization is prolonged, and treatment costs increase. For this reason, taking precautions for the risk factors of acute and chronic diseases and developing appropriate screening policies are seen as the first step in the management of diseases (6).
Many pharmacological and non-pharmacological methods are used to manage the physiopsychosocial change caused by acute or chronic diseases and to adapt individuals to the disease process. One of these methods is the laughter therapy, which has been frequently applied to healthy/sick individuals in every field for the last 10 years and scientific reports about its beneficial effects are increasing. Although the history of laughter therapy begins with psychiatrist Dr. William F. Fry, known as the father of geletology (the science of laughter), many scientists have contributed to its development (11). Laughter therapy is defined as a unique set of exercises that combines laughing without reason and pranamaya breathing technique. In particular, simulated laughter exercises were introduced in 1995 by Dr. Developed by Madan Kataria (12). Laughter therapy sessions begin with gentle warm-up techniques that include clapping, various body movements, and stretching. These facilitate the transition to childish playfulness. After these exercises, the sessions are completed with laughter and breathing exercises. Studies prove that our body does not distinguish between real and fake laughter and that at least 20 minutes of laughter therapy is sufficient to provide physiological, psychological and social benefits (12-14).
Laughter therapy is applied to large populations from children to the elderly, from individuals with chronic diseases such as cancer, chronic kidney failure, lung diseases, diabetes mellitus to healthy individuals. Laughter therapy is widely used to reduce pain, strengthen immunity, regulate blood glucose level, increase oxygenation level, reduce stress, improve quality of life, and control many symptoms related to illness or treatment (13,15-20).
Although there are many studies on the application of laughter therapy on different patient groups and healthy individuals, there are limited number of systematic reviews and meta-analysis studies on the subject. When the literature was reviewed, it was seen that there is a need for systematic reviews and meta-analyses showing the effectiveness of laughter therapy, which is seen to be effective in controlling physiological and psychological symptoms, on quality of life, anxiety, stress and sleep management (21-22). With the increase in the preferability of laughter therapy as a non-pharmacological method in the last 10 years, it was decided to conduct this study in order to present high-level evidence. In the light of the data obtained, it is thought that laughter therapy, which is cheap and easily applicable in sick individuals, will be more preferred in controlling a wide variety of physiological and psychological problems, reduce the long-term hospitalization times and costs for symptom control of patients, and increase their quality of life. It is expected that the results of the research will contribute to the national/international literature, nursing practices and future studies on laughter therapy.
The Aim of the Research and the Research Question
The aim of this systematic review and meta-analysis study is to determine the effect of laughter therapy applied to adult patients on anxiety, stress, sleep and quality of life. The research question sought to be answered in the study: What is the effect size of laughter therapy applied to adult patients on anxiety, stress, sleep and quality of life?
METHODS
Protocol and Registration
The protocol of this systematic review and meta-analysis study was registered on the PROSPERO database (CRD42023411896) and reported according to the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis Statement) protocol. (23). Ethics committee approval was not required as the data of the study would be obtained from studies published in the literature.
Eligibility Criteria
In this systematic review, studies meeting the inclusion/exclusion criteria were selected according to the PICOS (P: Population, I: Interventions, C: Comparisons, O: Outcomes, S: Study designs) format. (Table 1.)
Table 1. PICOS criteria for inclusion/exclusion of studies.
| Inclusion Criteria | Exclusion Criteria |
| Population-P: Adult patients | Population-P: Studies that did not include adult patients in the sample |
| Interventions-I: Lauhgter therapy | Interventions-I: Studies that do not include laughter therapy intervention, |
| Comparisons-C: Adult patients receiving laughter therapy and routine patient care steps | Comparisons-C: Studies without any comparison group and studies with more than two comparison groups |
| Outcomes-O: Somatic and mental effects (as defined in research such as quality of life, anxiety, stress and sleep problems) | Outcomes-O: Studies with no results on quality of life, anxiety, sleep and stress level, |
| Study designs-S: The article language is English and Turkish, randomized controlled experimental and quasi-experimental studies with full-text access are included. The research was carried out to cover the years between March 2013 and March 2023. | Study designs-S: Non-randomized controlled trials; Randomized controlled trials published as conference abstracts/scientific papers, letters to the editor or reviews are not included. |
Literature Search Strategy
This search was carried out over the period 09/03-09-04/2023 using Web of Science (WOS), Pubmed, Science Direct, Scopus, Cochrane, Proquest and YÖK-National Thesis Center databases. Turkish and English studies were scanned between March 2013 and March 2023. Within the framework of the research questions, a pre-screening was conducted using the terms Medical Subject Headings (MESH), mainly “adult patients”, “laughter therapy”, “laughter yoga” and related terms.
Selection of Studies
While scanning, the data obtained using MESH terms were transferred to the Mendeley program. Repeated studies (duplication) were determined and eliminated by the researcher (GK). The titles and summaries of the obtained studies were evaluated by two independent researchers (“GK” and “SK”) in line with the inclusion/exclusion criteria previously determined. Excluded studies were coded according to the reasons for exclusion. In case of inconsistency, full-text analysis was performed in the studies that were examined considering the publication language, study design, inclusion/exclusion criteria.
Data Extraction
The data extraction tool developed by the researchers was used. In the data extraction tool the name of the study, author/publication year/country, place and year of the study, study design, data collection tool, duration and frequency of laughter therapy, sample size, group characteristics (as defined in studies), physical and psychological symptoms (anxiety, sleep , stress levels), quality of life scores were obtained. The data extraction process was carried out manually by the researcher (“GK”) and controlled by the second consultant (“SK”).
Methodological Quality Evaluation of the Studies
Randomize controlled trails (RCTs) and quasi-experimental studies were included in this systematic review and meta-analysis. The methodological quality of the included studies was evaluated by checklists published by the Joanna Briggs Institute. Accordingly, the quality evaluation of randomized controlled studies was made with 13-item and quasi-experimental studies with nine-item checklists (24-26). Each item in these lists is evaluated as “yes, no, uncertain and inapplicable”. The methodological quality level of the studies included in the research was considered “mediocre” if less than 50% of the items were evaluated as “yes”; “moderate quality” if 51-80% of the items were evaluated as “yes”; and “good quality” if more than 80% of the items were evaluated as “yes”.
Synthesis of the Data
Meta-analysis was used in data synthesis in this systematic review. Comprehensive Meta-Analysis (CMA) 3.0 program was used for meta-analysis. “Cochran Q and Higgins I²” statistics were used to evaluate heterogeneity among studies in the meta-analysis. An I² rate exceeding 50% was accepted as an important indicator of heterogeneity. Accordingly, “Random Effect” results were considered if the studies showed heterogeneous distribution. In the study, the number of laughter therapy sessions was examined by subgroup analysis. The value of “Hedge’s g” was used for the overall effect size in the meta-analysis. The overall effect and subgroup effect sizes are shown with the forest plot. All statistical calculations were made at 95% confidence interval and 0.05 significance level.
RESULTS
Searching Results
In this study, the results of the scan yielded 1039 records from the databases; Web of Science (n=47), Pubmed (n=98), Science Direct (n=480), Scopus (n=118), Cochrane (n=159), YÖK-National Thesis Center (n=7) and Proquest (n=130) and 2 from other sources (n=2), a total of 1041 studies were obtained. After the repetitive data extraction, title and summary analysis, 26 studies were identified. As a result of full-text analyzes and inclusion/exclusion criteria, 16 studies were included in the meta-analysis. Reasons for exclusion from meta-analysis; PRISMA flowchart indicated that full-text language was within the exclusion criteria (n=3), no control group (n=2), more than two groups (n=3), and inappropriate statistical studies (n=2). (Figure 1).
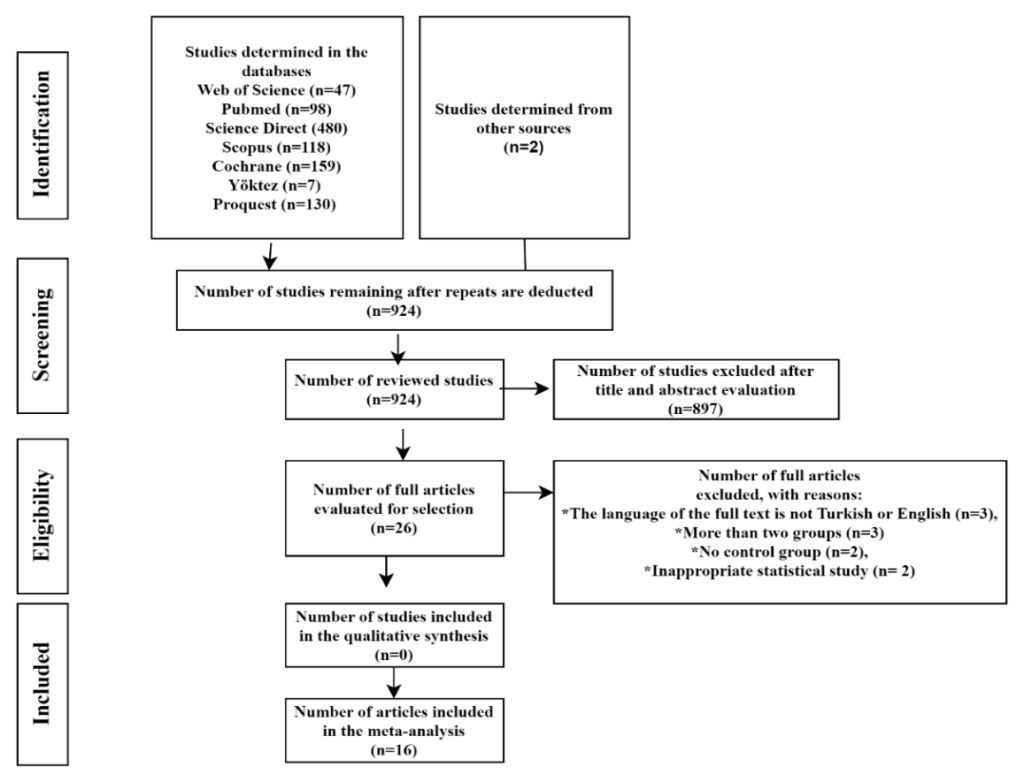
Figure 1. Prisma flow chart of scanning process.
Study Characteristics
Total of 16 studies included in this systematic review and meta-analysis; 7 of them are randomized controlled studies and 9 of them are quasi-experimental design studies. Studies were conducted in Turkey (n=3), Spain (n=1), the Middle East and Asia (Iran, n=5; Korea, n=4; Japan, n=2; Hong Kong, n=1). The total sample size of the studies included in the analysis was 1212 (Experimental Group: 650, Control Group: 562). The duration and frequency of laughter therapy application varied in the studies analyzed. In most of the studies, repeated applications and repeated measurements at different times were made in a minimum of 4 and a maximum of 16 sessions. The effect of laughter therapy on sleep quality in 2 studies; effect on stress, sleep and quality of life in 6 studies; effect on anxiety in 4 studies; effect on quality of life in 2 studies; effect on stress level in 2 studies were examined (15-18,27-38). The frequency and duration of laughter therapy application, the characteristics of the participants and detailed information are given in the table (Table 2).
Quality Assessment Results of the Studies
The metadological quality assessment levels of the studies analyzed are given in Table 2. As a result of the quality level evaluation, it was determined that five of the quasi-experimental studies had a medium quality level and four were mediocre; one of the randomized controlled experimental studies had a good quality level and six were medium quality level.
Table 2. Characteristics and main findings of the studies included in the systematic review and meta-analyses.
A: PSQI: Pittsburgh Sleep Quality Index, b: PSS:Perceived Stress Scale, c: HRQOL: Health-related quality of life, d: NRS:Numeric Rating Scale, e: HADS: Hospital Anxiety Depression Scale, f: BEPSI-K: Korean Brief Encounter Psychosocial Instrument, g: BAI: Beck Anxiety Inventory, h: DASS: Depression Anxiety Stress Scale, i: QSC-R23: Questionnaire on Stress in Cancer Patient, j: HSRS: Hospital Stress Rating Scale, k: FACT-G: The Functional Assessment of Cancer Therapy General, l: GDSSF-K: Geriatric Depression Scale Short Form, m: KDQOL-SF™: Kidney Disease Quality of Life Short Form, n: STAI-T: State-Trait Anxiety Inventory – Trait Form.
Results Of The Meta-Analysis
Sleep Quality
It was determined that studies were highly heterogeneous and the randomized effects model was used (Q=119,696, I2=96,658). The combined results of three studies (27,30,35) were examined according to the Hedge’s g effect size and the effect size was determined as g= -1.93 (95% CI=-3.768;-0.174, p=0.03<0.05). This result of the study shows that laughter therapy improves sleep quality in adult patients. The forest plot of the studies included in the meta-analysis is given in Figure 2.
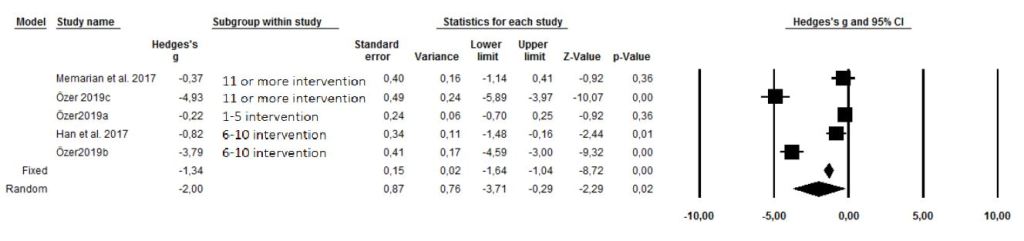
Figure 2. Forest plot- effect size of laughter therapy on sleep quality.
According to Classic Fail Safe-N statistical test, the number of studies obtained for the value of a=0.05 was found to be 141. This result shows that for publication bias to exist, there should be 141 studies with opposite values to the study findings included in the meta-analysis. Begg and Mazumdar Rank (p-value-2 tailed=0.08641>0.05) and Egger regression statistical test (p-value-2 tailed = 0.11126>0.05) were performed to evaluate publication bias. According to these statistical results, it was determined that there was no publication bias (Figure 3).
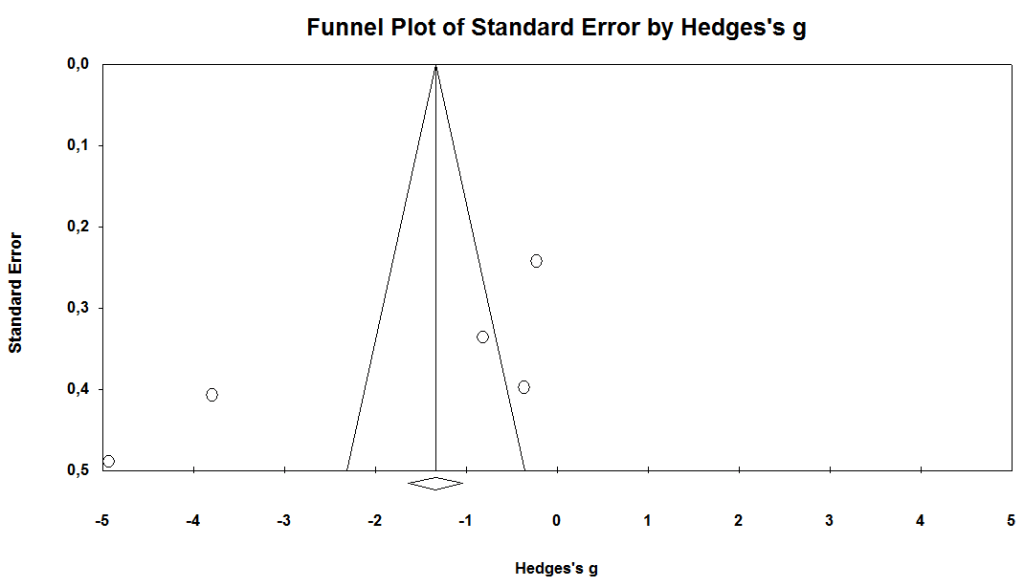
Figure 3. Funnel plot for sleep quality.
In this meta-analysis, subgroup analysis was conducted to explain the reason for heterogeneity. In subgroup analysis; since the number of interventions was different in the included studies, repetitive measurements after the intervention were grouped and evaluated. When the combined results of the studies according to the repetitive laughter therapy interventions were examined, 1-5 interventions (g= -0.22, Z=-0.92, p=0.36>0.05), 6-10 interventions (g= -2.30, Z=-1.54, p=0.12>0.05) and 11 or more interventions (g= -2.64, Z= -1.16, p=0.25>0.05) it was found that the sleep quality scores of the experimenatal groups were higher than the control groups, however these differences were not statistically significant. (Figure 4). It was observed that the total sleep quality scores of the experimental group increased after all interventions compared to the control group (g= -0.30, Z= -1.27, p=0.20>0.05). According to the effect sizes, it was determined that 11 or more interventions was the most effective number of intervention on sleep quality. (g= -2.64). Measurement results after 6-10 and 1-5 interventions, respectively, were also found to be effective (g= -2.30; g= -0.22). As a result of the analysis, it was seen that the number of laughter therapy interventions was effective on sleep quality, but the difference between the groups was not statistically significant (p>0.05).
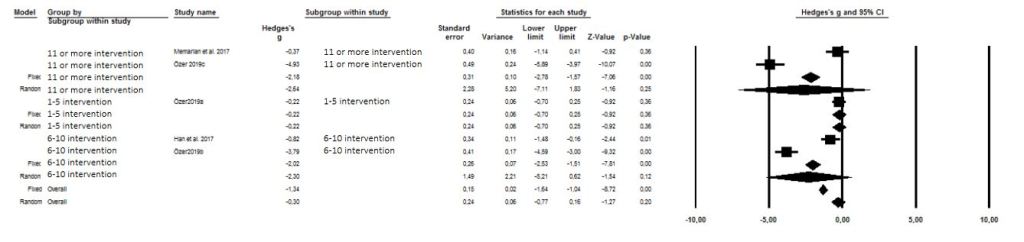
Figure 4. Forest plot – effect size of laughter therapy ıntervention numbers on sleep quality.
Anxiety
It was determined that studies were highly heterogeneous and the randomized effects model was used (Q=505,742, I2=98,616). The combined results of six studies (18,30,31,33,37,38) were examined according to the Hedge’s g effect size and the effect size was determined as g= -1.93 (95% CI=-3.768;-0.174, p=0.03<0.05).
This result of the study shows that laughter therapy reduces the level of anxiety in adult patients. The forest plot of the anxiety studies included in the meta-analysis is given in Figure 5.
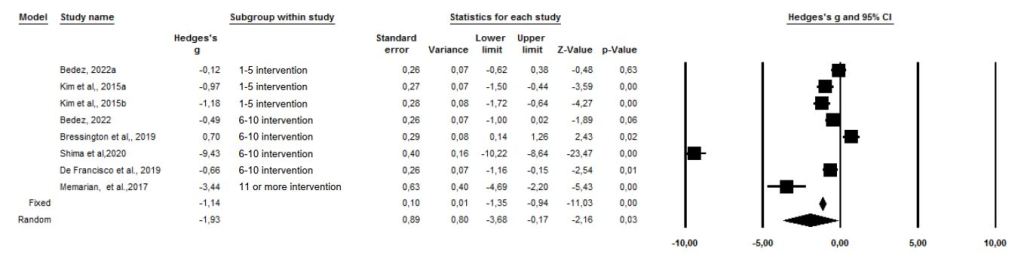
Figure 5. Forest plot – effect size of laughter therapy on anxiety level.
In this meta-analysis, Classic Fail Safe-N (393 studies obtained for a=0.05 value), Begg and Mazumdar Rank (p-value-2 tailed=0.1776>0.05) and Egger regression statistical test (p-value-2 tailed =0.11253>0.05) were performed to evaluate publication bias. According to these statistical results, it was determined that there was no publication bias (Figure 6).
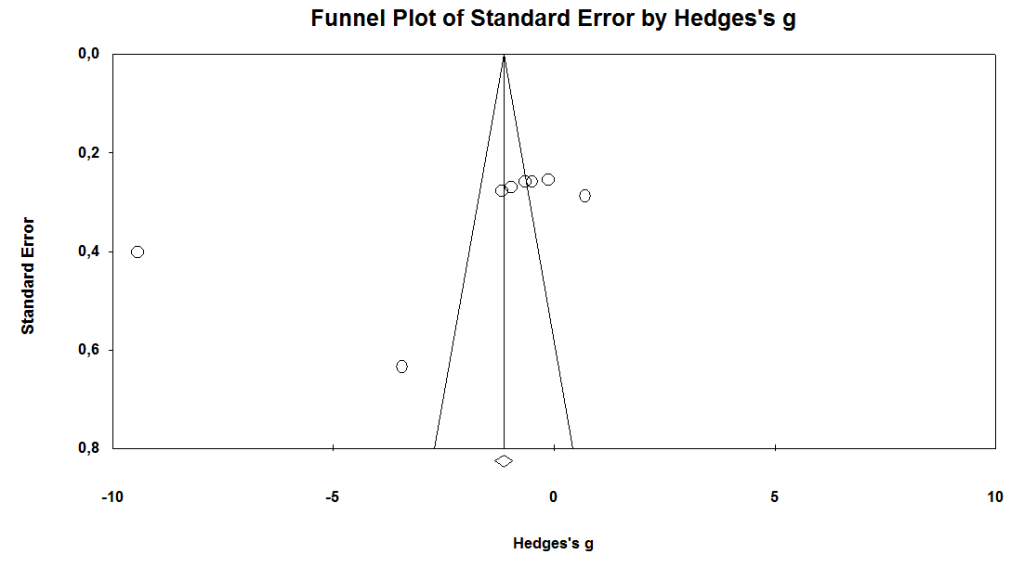
Figure 6. Funnel plot for anxiety level.
In the effect of laughter therapy on anxiety, 11 or more interventions were found to be the most effective number of applications (g= -3.44 p=0.00<0.05), followed by 6-10 interventions and 1-5 interventions, respectively. (g= -2.46 p=0.18>0.05; g= -0.75 p=0.02<0.05). Laughter therapy with 6-10 interventions was found to be effective, but not statistically significant. (p=0.18>0.05). According to the combined results of the studies, it has been determined that the laughter therapy reduces the anxiety levels of patients. (g= -1.35, Z=-4.68, p=0.00<0.05) (Figure 7.) In the included studies, according to the subgroup analysis of the number of laughter therapy interventions, the difference between the groups was found to be statistically significant (p=0.001<0.05).
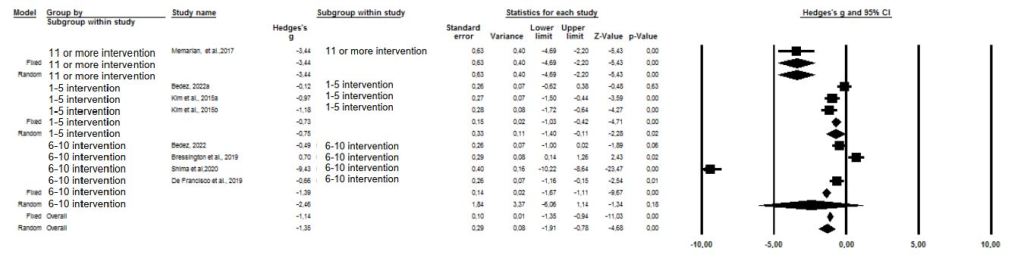
Figure 7. Forest plot – effect size of laughter therapy ıntervention numbers on anxiety level.
Stress
It was determined that studies were highly heterogeneous and the randomized effects model was used (Q=505,975, I2=98,221).The combined results of eight studies (15,18,28,31,33,34,36). were examined according to the Hedge’s g effect size and the effect size was determined as g= -1.704 (95% CI=-3.185;-0.223, p=0.000<0.05). This result of the study shows that laughter therapy reduces the level of stress in adult patients. The calculated effect sizes of the studies conducted in randomized controlled and quasi-experimental design are given in Figure 8.
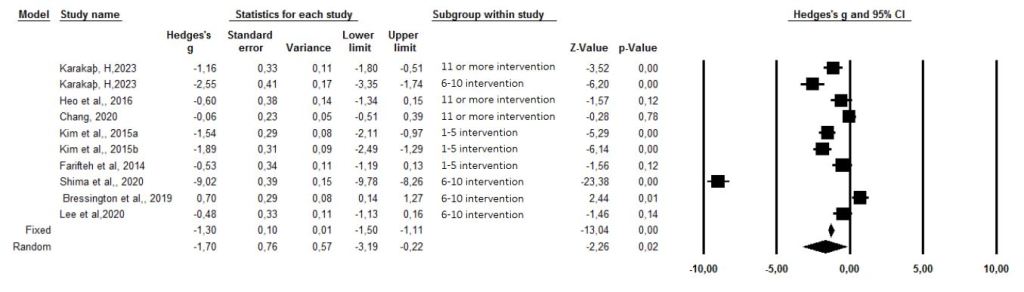
Figure 8. Forest plot – effect size of laughter therapy on stress level.
In this meta-analysis, Classic Fail Safe-N (565 studies obtained for a=0.05 value), Begg and Mazumdar Rank (p-value-2 tailed=0.08924>0.05) and Egger regression statistical test (p-value-2 tailed =0.11355>0.05) were performed to evaluate publication bias. According to these statistical results, it was determined that there was no publication bias (Figure 9).
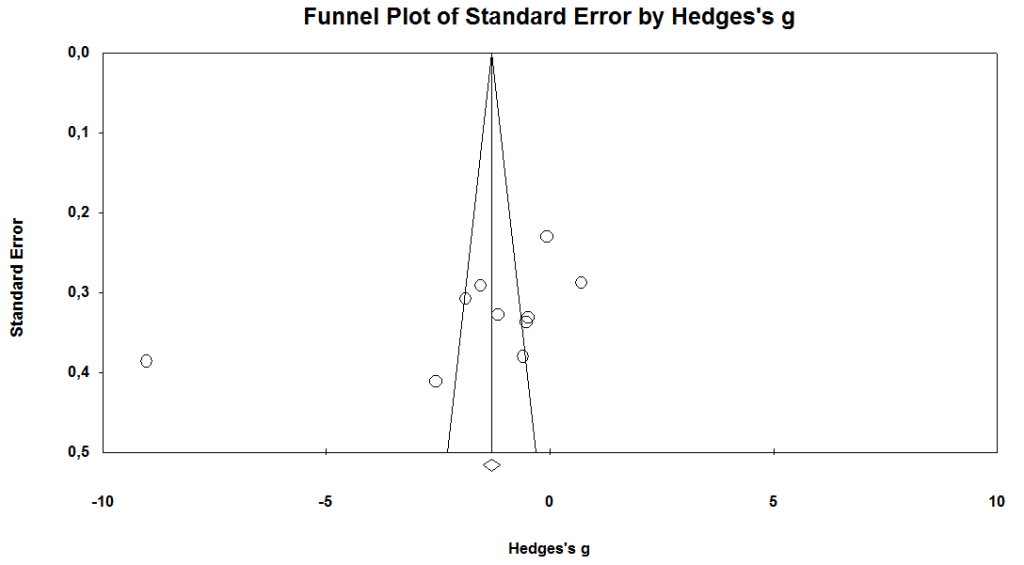
Figure 9. Funnel plot for stress level.
According to the combined results of the findings of the eight included studies; laughter therapy with 1-5 interventions was effective in reducing stress and was statistically significant (g= -1.33; Z=-3.40; p=0.00<0.05); according to 6-10 intervention and 11 or more intervention measurements, laughter therapy was found to be effective in reducing stress but it was not statistically significant (respectively g= -2.88; Z=-1.34; p=0.18>0.05 and g= -0.58; Z=-2.64; p=0.10>0.05). In total, it was found that the stress level score in the experimental group that received laughter therapy was statistically significantly lower than the control group. (g= -0.94; Z=-3.64, p=0.00<0.05) (Figure 10).

Figure 10. Forest plot – effect size of laughter therapy ıntervention numbers on stress level.
Quality of Life
It was determined that studies were highly heterogeneous and the randomized effects model was used (Q=206,479, I2=94,188). The combined results of seven studies (16,17,29,31,32,33,36) were examined according to the Hedge’s g effect size and the effect size was determined as g=0.712 (95% CI= 0.180;1.243, p= 0.009<0.05). According to combined results of the seven studies, it was found that the quality of life scores in the experimental group was statistically significantly higher than in the control group. The forest plot of the quality of life studies included in the meta-analysis is given in Figure 11.
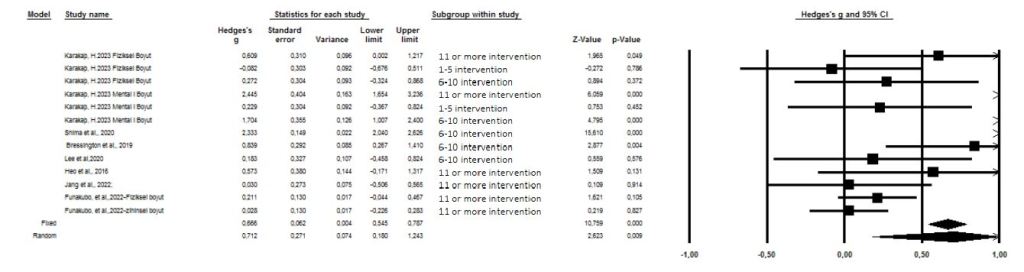
Figure 11. Forest plot – effect size of laughter therapy on life quality.
In this meta-analysis, Classic Fail Safe-N (338 studies obtained for a=0.05 value) and Egger regression statistical test (p-value-2 tailed=0.84643>0.05) were performed to evaluate publication bias. According to these statistical results, it was determined that there was no publication bias. Since p-value-2 tailed=0.04408 < 0.05 according to Begg-Mazumdar Rank test, it can be said that there was publication bias (Figure 12).
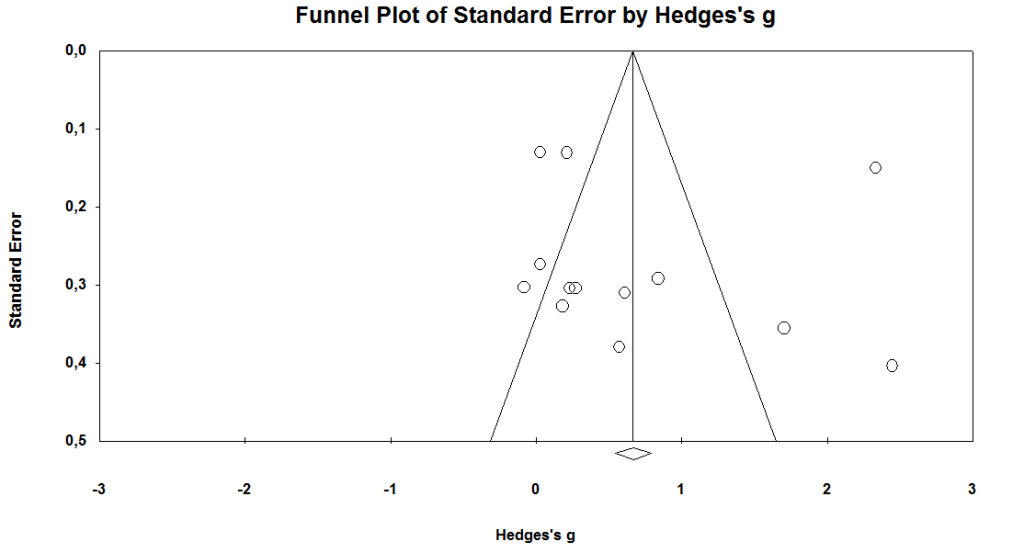
Figure 12. Funnel plot for life quality.
It was found that laughter therapy with 1-5 interventions was effective in increasing the quality of life, but it was not statistically significant. (g=0.073; Z=0.339; p=0.735>0.05). According to 6-10 intervention and 11 or more intervention measurements, laughter therapy was found to be effective in increasing quality of life and was statistically significant (respectively g=1.080; Z=2.169; p=0.030<0.05 and g=0.558; Z= 2.280; p=0.022<0.05). In the combined results of the study, it was found that the mean quality of life score in the experimental group that received laughter therapy was statistically significantly higher than the control group. (g=0.359; Z=2.344, p=0.019<0.05) (Figure 13).
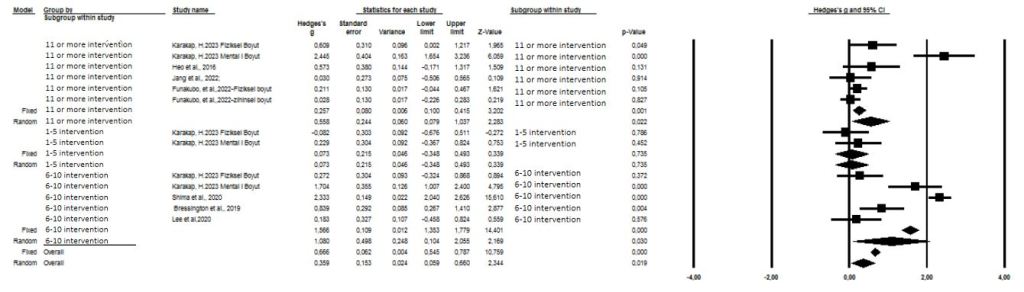
Figure 13. Forest plot – effect size of laughter therapy ıntervention numbers on stress level.
Side Effects of Laughter Therapy
It was reported as a side effect that it may lead to acute deterioration in pulmonary functions by causing hyperinflation in one study which was not included because the full text could not be accessed (39). However, there was no information on any side effect observed in the studies included in the study.
DISCUSSION
There are many studies in the literature examining the effect of laughter therapy on patients and healthy individuals (40-44). Laughter therapy has many positive effects on body physiology, such as reducing cortisol level, inducing the secretion of some immuglobins, endorphins and derivatives, accelerating circulation, strengthening immunity, improving sleep and life quality, increasing cellular oxygenation by increasing the tidal capacity of the lung, reducing pain, and relaxing muscles (32,40-44). In regular laughter therapy practices, a few minutes of laughter exercises can produce the same effects as rowing for about 15 minutes (45). In line with the literature results, this systematic review and meta-analysis study was conducted to determine the effect of laughter therapy on anxiety, stress, sleep and quality of life in adult patients, and the results of 16 studies that met the criteria were analyzed.
In this study, it was determined that laughter therapy was effective in reducing the level of anxiety and the effect size was related to the number of interventions. It was determined that 11 or more laughter therapy interventions significantly reduced the anxiety level compared to other intervention groups (1-5 and 6-10 interventions). Similar to the findings of this meta-analysis study, in a meta-analysis conducted by van der Wal and Kok in which studies involving laughter therapy were examined, it was reported that simulated laughter therapy was effective in reducing anxiety levels (22). In a meta-analysis examining the effect of laughter therapy on anxiety, it was reported that laughter therapy is an effective complementary method in reducing the level of anxiety (46). Similar results were found in the systematic review examining the effect of laughter therapy on anxiety in patients with breast cancer, it was emphasized that laughter therapy is an effective method in reducing anxiety (47). In the study conducted by Bedez (2019) with cancer patients; it was determined that as the number of laughter therapy interventions increased in the experimental group, the mean scores of anxiety levels decreased significantly (37). According to these results, it can be said that laughter therapy is a suitable alternative method that can be used in the management of anxiety in sick individuals.
In this systematic review and meta-analysis, it was found that laughter therapy applied to adult patients reduced the stress level in the experimental group, but there was no statistically significant difference in effect size related to the number of interventions. In a meta-analysis examining the effects of laughter therapy on stress level, laughter-inducing therapies have been reported to significantly reduce stress. In the meta-analysis conducted by Van der Wal and Kok (2019), it was emphasized that stress levels are based on different stress scales and cortisol measurements. Studies included in the meta-analysis reported that although laughter therapy reduces cortisol levels, the level of evidence for this is low (22). In the literature, it is seen that cortisol levels decrease significantly, especially after the fourth laughter therapy intervention (48,49). In a study included in the meta-analysis, it was reported that the mean stress level scores of the patients in the experimental group in which laughter therapy was applied significantly decreased after 8 and 16 interventions (6-10, 11 and more interventions) compared to the patients in the control group and the number of interventions was statistically significant in reducing the stress level. (28). These results suggest that laughter therapy should be used in the stress management of sick individuals. In addition, considering the studies on cortisol levels, it can be recommended that the number of laughter therapy interventions should be at least four times.
As a result of the meta-analysis study; It was seen that laughter therapy was effective in increasing the sleep quality of individuals, but there was no statistically significant difference in effect size related to the number of interventions. In another systematic review on the subject, laughter therapy was found to have a positive effect on improving sleep quality. (49). When the studies included in the meta-analysis were examined in terms of sleep quality, Özer (2019) reported that the average sleep quality score of experimental group, which was laughter therapy applied to hemodialysis patients 2 times a week for 8 weeks, 16 times in total, was lower and significant compared to the control group (27). In the study of Han et al. (2017), it was reported that laughter therapy, which was applied for 4 weeks, twice a week for 8 interventions, increased sleep quality. (35). According to the results of the meta-analysis, it can be said that laughter therapy can be applied to improve sleep quality in different patient groups.
According to the analysis results of this study, laughter therapy was found to be effective in improving the quality of life. The effect of laughter therapy is discussed according to the number of interventions. It was determined that the measurements after 1-5 laughter therapy interventions affected the quality of life but were not statistically significant, 6-10 and 11 or more laughter therapy interventions were significant in increasing the quality of life. Karakaş (2020), reported that laughter therapy applied to hemodialysis patients had higher life quality scores after the 8th and 16th interventions (28). The randomized controlled trial included in the meta-analysis reported that laughter therapy increased quality of life in patients with cancer (29). According to the combined analysis results of the study; laughter therapy increase the quality of life in different patient groups and this therapy can be used as a nursing intervention.
The strengths of the study are that there is no publication bias, literature review by two researchers, up-to-date sources, data are collected with reliable measurement tools in the studies, there are different patient groups in the included studies and the quality evaluation scores of the included studies are moderate and good.
Limitations of this study are that the studies included in the meta-analysis have a small sample size, blinding has not been done in most studies, the number of randomized controlled studies on the subject is small, the side effects of laughter therapy are not reported, the duration of laughter therapy and the frequency of interventions are different in studies.
CONCLUSION
In this systematic review and meta-analysis, it was determined that laughter therapy applied to sick individuals reduced anxiety and stress levels, and increased sleep quality and life quality. These study analyzes with research results meeting the inclusion criteria, it has been shown that laughter therapy reduces anxiety and stress in sick individuals, and increases sleep and quality of life. According to the combined results of the study, it was seen that the number of laughter therapy interventions changed the effect size on the symptoms discussed. Some studies in the literature support the results of this study on anxiety, stress, sleep and quality of life. As the number of laughter therapy intervention increases, the anxiety scores of the sick individuals decrease; sleep and quality of life scores increase.
- Laughter therapy is an easily accessible and cost-effective nonpharmacologic method which has positive physiological and psychological effects on patients.
- It is thought that laughter therapy can be applied as a nursing intervention as an effective non-pharmacological method for reducing patients’ symptoms.
- Laughter therapy can be included as a non-pharmacological intervention in all health institutions especially in complementary and alternative medicine application centers.
- With the further research, it is thought that laughter therapy will reduce post-surgical complications, length of hospitalization, care costs and workload of healthcare professionals.
- Certificate programs can be organized to increase the awareness of nurses about laughter therapy and their participation can be encouraged.
Conflict of interest
There is no conflict of interest between the authors.
Author Contributions:
Concept – G.K., S.K; Design – G.K., S.K.; Supervision – S.K.; Resources – G.K.; Data Collection and/or Processing – G.K., S.K.; Analysis and/or Interpretation – G.K., S.K.; Literature Search – G.K., S.K.; Writing Manuscript – G.K.; Critical Review – S.K.
Ethical Aspect of the Study
There is no risk of material/moral harm to the researchers in the literature review. The articles examined within the scope of the study were cited in the bibliography.
Ethical Permissions
Ethics committee approval was not required as the data of the study were obtained from studies published in the literature.
Financial Disclosure
The authors declared that this study received no financial support.
ORCIDs
GK: 0000-0002-9213-4924
SK: 0000-0002-5718-0669
REFERENCES
- Alimohammadi N, Taleghani F, Mohammadi E, Akbarian R. The nursing metaparadigm concept of human being in Islamic thought. Nursing inquiry. 2014;21(2):121–129. doi: 10.1111/nin.12040.
- Fawcett J. Contemporary Nursing Knowledge: Analysis and Evaluation of Nursing Models and Theories. F.A. Davis, Philadelphia; 2005.
- World Health Organization (WHO). What is the WHO definition of health? Accessed 11.01.2023. https://www.who.int/about/ who-we-are/frequently-asked-questions.
- Akdemir N. Kronik Hastalıklar ve Hemşirelik Bakımı. In: Akdemir N, Birol L, eds. İç Hastalıkları ve Hemşirelik Bakımı [Chronic Diseases and Nursing Care. In: Internal Medicine and Nursing Care] Geliştirilmiş 3rd Ed., Ankara, Turkey. Sistem Ofset; 2011.
- Gülseven B, Oğuz S. Kronik Durumlar. İçinde: Karadakovan A, Aslan FE eds. Dahili ve Cerrahi Hastalıklarda Bakım [Chronic Conditions. In: Care in Internal and Surgical Diseases.] Geliştirilmiş 3. Baskı, Ankara, Akademisyen Tıp Kitabevi; 2014.
- World Health Organization (WHO). Noncommunicable Diseases. WHO Document Production Services, Geneva, Switzerland. Accessed 03.01.2023. https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
- Republic of Turkey Ministry of Health, General Directorate of Public Health (2021). Türkiye Bulaşıcı Olmayan Hastalıklar ve Risk Faktörleri Kohort Çalışması [Türkiye Non-Communicable Diseases and Risk Factors Cohort Study], Ankara. Accessed 19.01.2023. https://hsgm.saglik.gov.tr/depo/birimler/kronik-hastaliklar-engelli db/hastaliklar/kalpvedamar/raporlar_ist/v9s_NCD.kohort._27.10.2021.pdf
- Goldbeck L. The impact of newly diagnosed chronic paediatric conditions on parental quality of life. Quality of Life Research. 2006;15(7):1121-1131.
- Sturms LM, van der Sluis CK, Stewart RE, Groothoff JW, ten Duis HJ, Eisma WH. A prospective study on paediatric traffic injuries: health-related quality of life and posttraumatic stress. Clin Rehabil. 2005;19: 312-322.
- Türkmen E. Kronik Hastalıklar ve Önemi. İçinde: Durna Z, ed. Kronik Hastalıklar ve Bakım [Chronic Diseases and Their Importance. In: Chronic Diseases and Care] İstanbul, Nobel Tıp Kitabevleri; 2012
- Fry WF. The physiologic effects of humor, mirth, and laughter. JAMA. 1992;267(13):1857–1858. doi: 10.1001/jama.267.13.1857.
- Kataria M. Certified laughter yoga teacher training manual. (Guide) Bangalore: Laughter Yoga International University; 2019.
- Bennett PN, Parsons T, Ben-Moshe R, et al. Intradialytic Laughter Yoga therapy for haemodialysis patients: a pre-post intervention feasibility study. BMC complementary and alternative medicine. 2015;15:176. doi: 10.1186/s12906-015-0705-5.
- Ripoll RM, Casado IQ. Laughter and positive therapies: modern approach and practical use in medicine. Revista de psiquiatria y salud mental. 2010;3(1):27–34. doi: 10.1016/S1888-9891(10)70006-9.
- Farifteh S, Mohammadi-Aria A, Kiamanesh A, Mofid B. The Impact of Laughter Yoga on the Stress of Cancer Patients before Chemotherapy. Iranian journal of cancer prevention. 2014;7(4):179–183.
- Funakubo N, Eguchi E, Hayashi R, et al. Effects of a laughter program on body weight and mental health among Japanese people with metabolic syndrome risk factors: a randomized controlled trial. BMC geriatrics. 2022;22(1):361. doi: 10.1186/s12877-022-03038-y
- Jang KS, Oh JE, Jeon GS. Effects of Simulated Laughter Therapy Using a Breathing Exercise: A Study on Hospitalized Pulmonary Tuberculosis Patients. International journal of environmental research and public health. 2022;19(16):10191. doi: 10.3390/ijerph19161
- Kim SH, Kim YH, Kim HJ. Laughter and Stress Relief in Cancer Patients: A Pilot Study. Evidence-based complementary and alternative medicine: eCAM. 2015;864739. doi: 10.1155/2015/864739
- Field T. Yoga clinical research review. Complementary therapies in clinical practice. 2011;17(1):1–8. doi: 10.1016/j.ctcp.2010.09.007
- M. Čokolič M, Stangler Herodez Š, Sternad S, Krebs S. The inhibitory effect of laughter yoga on the increase in postprandial blood glucose in type 2 diabetic patients. Diabetologia Croatica. 2013;42:54-58.
- Stiwi K, Rosendahl J. Efficacy of laughter-inducing interventions in patients with somatic or mental health problems: A systematic review and meta-analysis of randomized-controlled trials. Complementary therapies in clinical practice. 2022; 47:101552. doi: 10.1016/j.ctcp.2022.101552
- van der Wal CN, Kok RN. Laughter-inducing therapies: Systematic review and meta-analysis. Social science & medicine. 2019; 232:473–488. doi: 10.1016/j.socscimed.2019.02.018
- Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. International journal of surgery (London, England). 2010;8(5): 336–341. doi: 10.1016/j.ijsu.2010.02.007.
- The Joanna Briggs Institute. The Joanna Briggs Institute critical appraisal tools for use in JBI systematic reviews: checklist for qualitative research, 2017. Accessed 01.03.2023. https://jbi.global/sites/default/files/2019-05/JBI_RCTs_Appraisal_tool2017_0.pdf.
- Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp, L. Explanation for the critical appraisal tool for RCTs with individual participants in parallel groups. In: Aromataris, E, Munn, Z., editors. JBI Manual for Evidence Synthesis. JBI, (2020a). Accessed 01.03.2023. https://synthesismanual.jbi.global. doi: 10.46658/JBIMES-20-04.
- Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Explanation for the critical appraisal tool for Quasi-Experimental Studies (experimental studies without random allocation). In: Aromataris E, Munn Z, editors. JBI Manual for Evidence Synthesis. JBI, (2020b). Accessed 01.03.2023. https://synthesismanual.jbi.global.
- Özer Z. Kahkaha Yogasının Hemodiyaliz Tedavisi Uygulanan Hastalarda Plazma Beta Endorfin Düzeyine, Ağrı Şiddetine ve Uyku Kalitesine Etkisi [The effects of “laughter yoga” on the plasma beta-endorphin levels, pain levels and sleep quality of hemodialysis patients.] [PhD Thesis]. Üsküdar Üniversitesi;2019.
- Karakaş H. Meme Kanserli Kadinlara Uygulanan Gülme Terapisinin Algilanan Stres Düzeyi ve Yaşam Kalitesine Etkisi [The Effect Of Laughter Therapy On Perceived Stress Level And Qualıty Of Life In Women With Breast Cancer] [(Master Thesis]. İzmir Bakırçay Üniversitesi;2023
- Morishima T, Miyashiro I, Inoue N, et al. Effects of laughter therapy on quality of life in patients with cancer: An open-label, randomized controlled trial. PloS one. 2019;14(6):e0219065. doi: 10.1371/journal.pone.0219065.
- Memarian A, Sanatkaran A, Bahari S. The effect of laughter yoga exercises on anxiety and sleep quality in patients suffering from Parkinson disease. Biomedical Research and Therapy. 2017;4(07): 1463-1479. doi: 10.15419/bmrat.v4i07.200doi: 10.15419/bmrat.v4i07.200
- Bressington D, Mui J, Yu C, Leung SF, Cheung K, Wu CST, et al. Feasibility of a group-based laughter yoga intervention as an adjunctive treatment for residual symptoms of depression, anxiety and stress in people with depression. Journal of affective disorders. 2019;248:42–51.
- Lee YJ, Kim MA, Park HJ. Effects of a laughter programme with entrainment music on stress, depression, and health-related quality of life among gynaecological cancer patients. Complementary therapies in clinical practice. 2020;39:101118. doi: 10.1016/j.ctcp.2020.101118
- Shima Rouhi S, Etemadi S, Pooraghajan M. Laughter in combination with yoga exercises: Changes in psychological distress and quality of life in patients with coronary heart disease (CHD). The Open Psychology Journal. 2020;13:144-150. 10.2174/1874350102013010144.
- Chang MY. Effects of a tai chi exercise program incorporating laughter therapy on the blood pressure, stress response and depression of older people with hypertension. Asia Life Sciences. 2019;Suppl19(2):93-101.
- Han JH, Park KM, Park H. Effects of laughter therapy on depression and sleep among patients at long-term care hospitals. Korean Journal of Adult Nursing. 2017;29(5):560-568. doi:10.7475/kjan.2017.29.5.560.
- Heo EH, Kim S, Park HJ, Kil SY. The effects of a simulated laughter programme on mood, cortisol levels, and health-related quality of life among haemodialysis patients. Complementary therapies in clinical practice. 2016;25:1–7. doi: 10.1016/j.ctcp.2016.07.001
- Bedez G. Hematolojik kanser hastalarında kahkaha yogasının bulantı kusma ve anksiyete üzerine etkisi [The effect of laughter yoga on nausea, vomiting and anxiety in hematological cancer patients.] [PhD Thesis]. Dokuz Eylül Üniversitesi;2022.
- De Francisco S, Torres C, De Andrés S, et al. Effectiveness of Integrative Laughter Therapy to Reduce Anxiety, Improve Self-Esteem and Increase Happiness: A Naturalistic Study at a Day Hospital for Addictive Disorders. International journal of environmental research and public health. 2019;16(21):4194. doi: 10.3390/ijerph16214194
- Lebowitz KR, Suh S, Diaz PT, Emery CF. Effects of humor and laughter on psychological functioning, quality of life, health status, and pulmonary functioning among patients with chronic obstructive pulmonary disease: a preliminary investigation. Heart & lung: the journal of critical care. 2011;40(4):310–319. doi: 10.1016/j.hrtlng.2010.07.010.
- Fujisawa A, Ota A, Matsunaga M, et al. Effect of laughter yoga on salivary cortisol and dehydroepiandrosterone among healthy university students: A randomized controlled trial. Complementary therapies in clinical practice. 2018;32:6–11. doi: 10.1016/j.ctcp.2018.04.005
- Hirosaki M, Ohira T, Kajiura M, et al. Effects of a laughter and exercise program on physiological and psychological health among community-dwelling elderly in Japan: randomized controlled trial. Geriatrics & gerontology international. 2013;13(1):152–160. doi: 10.1111/j.1447-0594.2012.00877.x.
- Miles C, Tait E, Schure MB, Hollis M. Effect of Laughter Yoga on Psychological Well-being and Physiological Measures. Advances in mind-body medicine. 2016;30(1):12–20.
- Bennett PN, Hussein WF, Reiterman, M, Yu J, Schiller B. The effects of laughter therapy on depression symptoms in patients undergoing center hemodialysis: A pragmatic randomized controlled trial. Hemodialysis international. International Symposium on Home Hemodialysis. 2020;24(4):541–549. doi: 10.1111/hdi.12870.
- Sakai Y, Takayanagi K, Ohno M, Inose R, Fujiwara H. A trial of improvement of immunity in cancer patients by laughter therapy. Japan-hospitals: the journal of the Japan Hospital Association. 2013;(32):53–59.
- Keykhai Hosseinpour A. Laughter yoga exercises on psychomotor effects of Parkinson’s patients. [Graduate thesis] Isfahan University Faculty of Physical Education and Sport Sciences;2013.
- Demir Doğan M. The Effect of Laughter Therapy on Anxiety: A Meta-analysis. Holistic nursing practice. 2020;34(1):35–39. doi: 10.1097/HNP.0000000000000363.
- Ilkhani M, Mohtashami J, Rezaei H. Effect Of Laughter Therapy On Cancer-Related Anxiety in Patients With Breast Cancer; A Systematic Review. Journal of Advanced Pharmacy Education & Research. 2019;9(2):195.
- Tanaka A, Tokuda N, Ichihara K. Psychological and physiological effects of laughter yoga sessions in japan: A pilot study. Nursing and Health Sciences. 2018;20(3):304-312. doi:10.1111/nhs.12562
- Üner E, Sezer Balcı A. Kadıoğlu H. The Effect of Laughter Therapy on Physical and Mental Health: Systematic Review. Halk Sağlığı Hemşireliği Dergisi. 2022;4(3):251-269. DOI: 10.54061/jphn.1102843.
